

Emergency department coding is under growing pressure in 2026. Making even small documentation or coding errors can be costly. The 7 biggest emergency department coding mistakes affecting reimbursement in 2026 are:
- Incorrect E/M level selection
- Missing Modifier 25
- Critical care documentation failures
- Unbundling errors
- ICD-10 specificity gaps
- Observation status miscoding
- Consultation code misuse
According to ACEP’s release on insurer tactics and emergency care sustainability (2025), “Insurers use delaying, denying, reducing, and underpaying tactics that threaten emergency care”
These payer practices put more financial pressure on emergency departments. That’s why accurate documentation, correct coding, and payer rule compliance are essential.
Mistake #1: Incorrect E/M Level Selection
Incorrect E/M Level Selection can happen in two directions:
- Upcoding: billing a higher level than documentation supports
- Undercoding: billing a lower level than clinical complexity warrants.
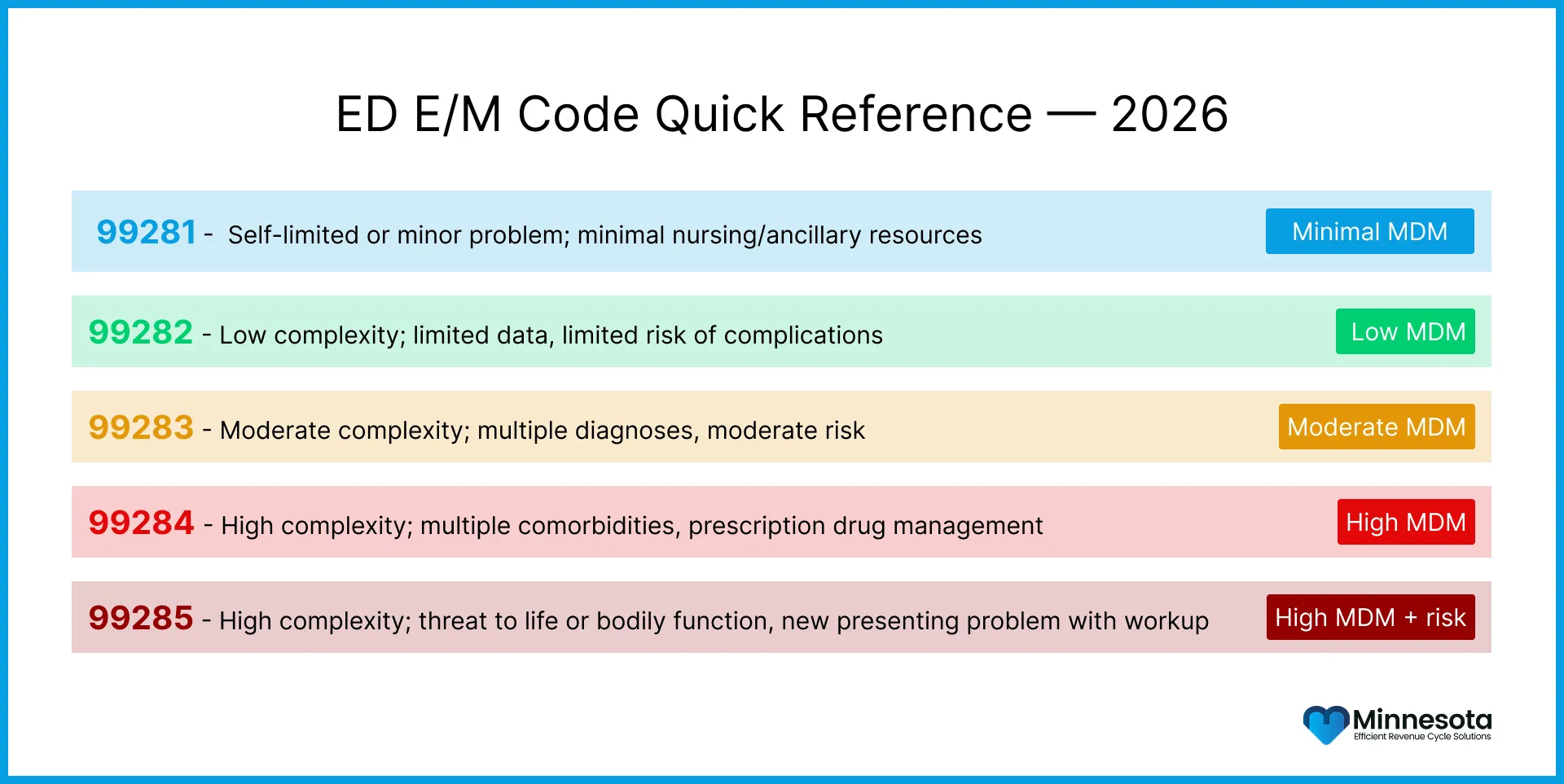
According to AMA’s 2026 E/M coding guidelines, code is selected on the basis of Medical Decision Making (MDM) and time. In this system, CPT codes 99281–99285 represent increasing levels of MDM complexity. Payers now use automated claim review algorithms to detect mismatches between documented MDM and billed codes.
A frequent coding mistake happens when coders select an E/M level on the basis of the physician’s subjective impression of how sick the patient appears. Instead, the code should be chosen on the basis of these factors:
- Problem complexity
- Reviewed data
- Risk of complications
How To Avoid Undercoding Or Overcoding E/M Services?
Follow these steps based on structured documentation in Medical Decision Making to code accurately:
- Document all 3 MDM elements clearly
- Validate moderate-complexity criteria (CPT 99284)
- Match the documented MDM level directly with CPT 99281–99285 selection
- Implement regular coder and clinician training aligned with American Medical Association CPT E/M Guidelines
Mistake #2: Missing or Misused Modifier 25
Modifier 25 is used when a significant, separately identifiable E/M service is performed on the same day as a procedure.
It happens because evaluation is often performed together with procedures like laceration repair, fracture reduction, or IV infusion. The Modifier 25 is very important and this is why it is also frequently audited.
According to CPT Modifier 25 rules, payers accept this modifier only when the E/M service is independent. It must not be part of the procedure work itself. The E/M must clearly show separate clinical decision-making beyond the procedure-related assessment.
Common Errors
- Applying Modifier 25 when there is no separate E/M note apart from the procedure note
- Using Modifier 25 for routine pre-procedure checks that are already included in the procedure payment
- Not using Modifier 25 when a separate E/M service is actually provided, leading to missed payment
How to Avoid Misused CPT Modifier 25?
Follow these steps accurately to use CPT Modifier 25:
- Write an E/M note that is separate from the procedure note.
- Include full problem assessment, clinical reasoning, and treatment plan
- Clearly document why the E/M service was medically necessary
- Use Modifier 25 only when a true separate E/M service is supported
Mistake #3: Critical Care Documentation Failures
99291 and 99292 are the highest-value critical care reimbursement codes. That value makes them the most strictly audited code pair in 2026.
A major documentation issue is faced when CPT and CMS rules are confused. These codes differ on timing:
- CPT rules: 99292 can be reported once 75 minutes is reached.
- CMS rules (Medicare): 99292 may only be reported when an additional 30 minutes is met. It requires about 104 total minutes before reporting.
If you are using CPT timing rules for CMS ,there is a high denial risk. To avoid this, clearly document the total critical care minutes delivered. Also, document the clinical severity, since critical care requires evidence of acuity, not routine monitoring.
In addition, CMS does not allow billing both ED E/M and CPT 99291 for the same provider on the same date. Doing this can trigger RAC recoupment.
How To Avoid Critical Care Documentation Failures?
- Use separate documentation templates for CMS and commercial payer critical care rules
- Document total critical care minutes clearly and explicitly in every case
- Subtract time spent on separately billable procedures before finalizing critical care time
- Train coders to verify payer-specific critical care rules before claim submission
Mistake #4: Unbundling and Bundling Errors
The CMS Correct Coding Initiative (CCI) edits define which procedure codes must be bundled together. These codes cannot be billed separately. When separate codes are billed for services that are already included in one comprehensive code, it is called unbundling. It causes lower reimbursement and increases compliance risk. Unbundling is a common emergency department coding error where
Common examples of unbundling are:
- Billing separate codes for wound irrigation and closure when a single repair code covers both
- Separately billing moderate sedation with a procedure that includes sedation in its global code
- Reporting individual components of a cardiovascular monitoring service that is already bundled into critical care
How To Fix Bundling And Unbundling Errors?
- Check CMS CCI edits before billing claim
- Review updated CMS CCI edit tables quarterly
- Train your coders on bundled vs separately billable procedure codes
- Use Modifier 59 or X-modifiers only when proper unbundling is justified
Mistake #5: ICD-10-CM Specificity Gaps
ICD-10-CM coding requires high diagnostic specificity. In ED unspecified diagnosis codes are common because documentation is often rapid and shorthand. However, in 2026, payers are using automated claim review systems. These systems flag low-specificity diagnoses when the documentation is vague. They downcode or deny claims if a more specific diagnosis is supported in the medical record.
Common ICD-10-CM Specificity Errors
3 high-frequency ICD-10 specificity errors in ED billing are :
- Laterality: Using R07.9 (unspecified chest pain) when a more specific chest pain type is documented.
- Injury site: Coding fractures as unspecified even when the exact bone and location are clearly documented
- Acuity: Using chronic or unspecified asthma codes when the visit clearly shows an acute asthma exacerbation
According to the ICD-10-CM code updates (October 1, 2025), “Practices that have not updated their code libraries or provider documentation templates may be systematically undercoding”.
How to Improve ICD-10-CM Specificity
- Use structured EHR prompts
- Cross-check physician notes against the most specific available diagnosis codes before billing
- Update coding knowledge yearly
Mistake #6: Observation Status Miscoding
Observation care in Emergency Medicine applies when a patient needs ongoing monitoring but does not meet inpatient admission criteria. Under CMS rules, observation services use separate CPT codes. They also have different reimbursement rates compared to standard ED E/M visits. However, a common error in coding practice that leads to denials is when:
Observation encounters are billed as ED visits or ED visits are billed as observation care.
A CMS analysis found that a significant portion of inpatient admission improper payments would have been payable if billed correctly. This shows that error flows in both directions
- Under-billing: This happens when a true observation encounter is coded as a standard ED E/M visit. It results in a lower facility payment.
- Over-billing: This occurs when inpatient admission codes are used for patients who only meet observation criteria. This can lead to repayment demands.
How to Improve Observation Coding in Emergency Medicine
- Set clear clinical criteria for observation. It should be based on documented medical reasoning, not bed assignment
- Make sure the physician and facility billing match for the same encounter
- Review CMS Two-Midnight Rule before deciding observation vs admission in borderline cases
Mistake #7: Misuse of Consultation Codes in the ED
In Emergency Medicine coding, outpatient consultation codes (99241–99245) are mostly incorrectly billed for specialist evaluation. These consultation codes were eliminated by CMS for payment. They are no longer reimbursed in the Medicare program. As a result, most commercial payers have also stopped recognizing these codes. When used in the ED setting, they lead to denial and compliance risk.
The correct approach is to report specialist consultations using standard ED E/M codes (99281–99285). These codes should reflect the actual complexity of the work performed.Both providers can bill separately when they perform distinct services. This is applicable only when each provider documents an independent assessment and avoids duplicating the same work.
How to Ensure Proper Consultation Billing?
- Confirm payer rules for consultation reporting before submitting any claim
- Ensure specialist providers document a clear and independent clinical assessment
- For out-of-network cases, check compliance with No Surprises Act
- Verify Qualified Payment Amount (QPA) calculations and IDR eligibility before billing
Table: 2026 ED Coding Risk Matrix
| Coding Error | CPT/Code Involved | Risk Level | Typical Impact | Primary Fix |
| Wrong E/M level selection | 99281–99285 | High | Denial or downcode on 10–20% of ED claims | Document all 3 MDM elements explicitly |
| Missing or misused Modifier 25 | E/M + procedure | High | Loss of E/M reimbursement on procedure-day visits | Separate, independent E/M documentation required |
| Critical care timing errors | 99291, 99292 | High | Automatic denial for Medicare; RAC recoupment risk | CMS vs. CPT timing templates; explicit minute count |
| Unbundling/bundling errors | Procedure pairs | Medium | Denial + compliance risk; or lost unbundled revenue | CCI edit review pre-submission |
| ICD-10 specificity gaps | Unspecified ICD codes | Medium | Downcode or denial for medical necessity | EHR specificity prompts; annual code update training |
| Observation status miscoding | Observation vs. ED codes | Medium | Under-billing or RAC repayment demand | Two-Midnight Rule criteria + physician alignment |
| Consultation code misuse | 99241–99245 (ED) | Lower | Claim rejection; NSA exposure for out-of-network | Use ED E/M (99281–99285) for specialist visits |
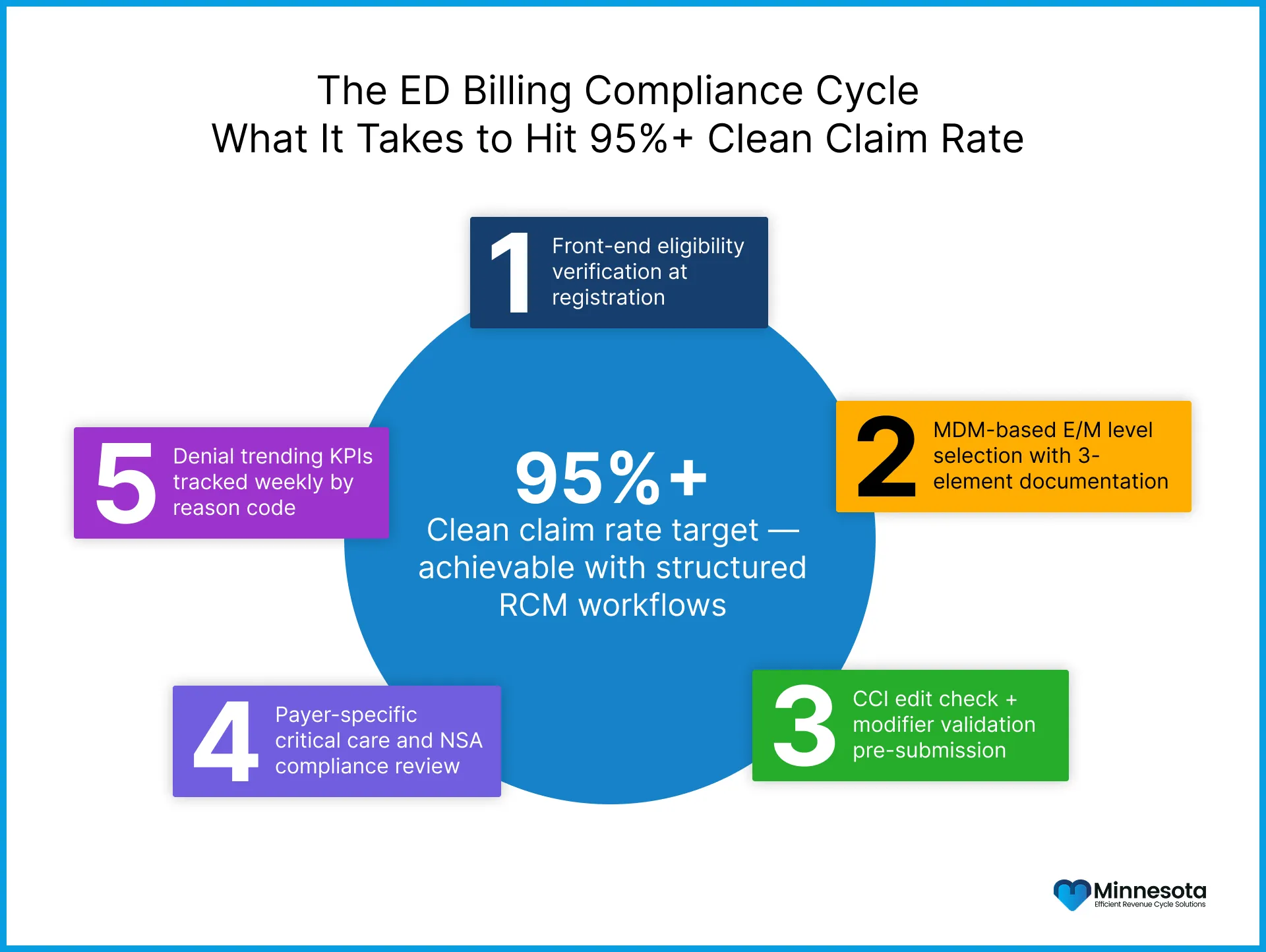
How Minnesota Billing Services Addresses These ED Coding Errors
Minnesota Billing Services specializes in revenue cycle management for emergency departments across Minnesota and the broader Midwest. Our team tracks weekly updates from CMS, AMA, and ACEP. We apply the most current MDM, and critical care rules to every claim.
Frequently Asked Questions
1. What are the major causes of ED claim denials in 2026?
Incorrect E/M level selection and missing documentation of MDM elements are the most common causes.
2. Why is Modifier 25 often denied in ED billing?
It is denied when the E/M note is not separate from the procedure note or lacks independent medical decision-making.
3. How is ED critical care time calculated correctly?
Critical care time must include total minutes only, excluding separately billable procedure time.
4. Can consultation codes still be used in emergency departments?
No, most payers including Medicare no longer reimburse 99241–99245 in ED settings. Use ED E/M codes instead.